
Can LPR Cause Cancer? Expert Insights Here
Laryngopharyngeal reflux, commonly abbreviated as LPR, is a condition where stomach acid travels backward into the larynx and pharynx, causing irritation and inflammation. Unlike gastroesophageal reflux disease (GERD), which primarily affects the esophagus, LPR reaches higher into the throat and voice box. Many people experiencing persistent hoarseness, chronic cough, or throat clearing wonder about the long-term health implications of this condition. The question of whether LPR can cause cancer is one that concerns patients and healthcare providers alike, particularly those managing this condition for extended periods.
Understanding the relationship between chronic acid reflux and cancer risk requires examining scientific evidence, cellular changes, and expert medical perspectives. While LPR is generally a manageable condition, chronic exposure to stomach acid can trigger significant changes in throat tissue. This comprehensive guide explores the cancer risk associated with LPR, how long it takes for potential malignant changes to develop, and what preventive measures you can take to protect your health. Whether you’re experiencing LPR symptoms or simply want to understand the medical science behind this condition, this article provides evidence-based insights from medical professionals and research institutions.

Understanding LPR and Acid Reflux Basics
Laryngopharyngeal reflux occurs when the lower esophageal sphincter (LES), a muscular ring that normally prevents stomach contents from flowing backward, becomes weakened or relaxes inappropriately. This allows gastric juices containing hydrochloric acid and pepsin to flow upward into the throat, voice box, and sometimes even the nasal passages. The condition differs fundamentally from typical heartburn because patients often don’t experience the burning sensation in the chest that characterizes GERD. Instead, LPR sufferers report symptoms like chronic hoarseness, persistent throat clearing, globus sensation (feeling of a lump in throat), and difficulty swallowing.
The throat tissues are far more sensitive to acid exposure than esophageal tissue, which has evolved protective mechanisms against acid. When stomach acid repeatedly contacts the delicate laryngeal and pharyngeal tissues, inflammation develops quickly. This chronic irritation is what prompts concerns about cancer development. The severity of LPR varies widely among individuals; some people experience occasional symptoms while others deal with constant throat discomfort. Understanding the basic mechanism of LPR is essential for comprehending how long-term acid exposure might lead to tissue changes that could potentially become cancerous.
Common triggers for LPR include late-night eating, spicy foods, caffeine, alcohol, obesity, and certain medications. Unlike GERD, which can often be managed with dietary changes alone, LPR frequently requires pharmaceutical intervention and lifestyle modifications. When considering whether LPR causes cancer, it’s important to recognize that the condition itself is not inherently cancerous, but chronic acid exposure creates an environment where cellular changes can occur over extended periods.
The Cancer Risk Connection: What Research Shows
Medical research has established a clear connection between chronic acid reflux and increased cancer risk, though the relationship is more complex than simple cause-and-effect. The American Cancer Society acknowledges that chronic GERD and LPR can increase the risk of certain cancers, particularly laryngeal and pharyngeal cancers. However, it’s crucial to understand that increased risk does not mean inevitable cancer development. Studies show that while patients with chronic reflux have higher cancer rates than the general population, the absolute risk remains relatively low when proper management occurs.
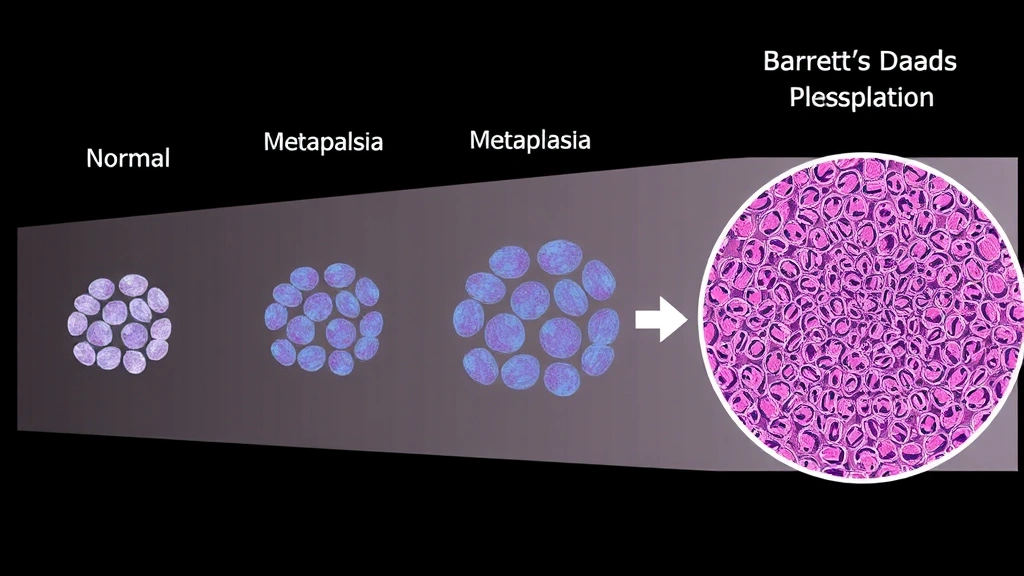
Research published in medical journals demonstrates that repeated acid exposure causes metaplasia—a process where normal cells transform into different cell types better suited to resist acid. While this adaptive response initially protects tissue, it can eventually lead to dysplasia, where cells become abnormal. If dysplasia progresses unchecked, it may eventually transform into cancer. This multi-step process typically requires years or even decades to develop, which is why the timeline matters significantly when discussing LPR and cancer risk.
The International Agency for Research on Cancer (IARC) has classified chronic reflux as a risk factor for esophageal and gastric cancers. Studies examining patients with long-standing LPR show that those with untreated or poorly managed reflux have elevated cancer rates compared to control groups. However, patients who actively manage their condition through medication, lifestyle changes, and regular monitoring show significantly reduced cancer risk. This finding underscores the importance of early detection and consistent management.
How Long Does LPR Take to Cause Cancerous Changes
The timeline for LPR to potentially cause cancer is highly variable and depends on numerous individual factors. Medical experts generally agree that cancer development from chronic reflux is not a rapid process. Most research suggests that significant cellular changes requiring years of continuous acid exposure are necessary before cancerous transformation occurs. In studies of patients with chronic GERD and LPR, the average time from initial diagnosis to development of Barrett’s esophagus or dysplasia ranges from 5 to 20 years, though this varies considerably.
For laryngeal and pharyngeal cancers specifically related to LPR, the timeline appears even longer. Many patients with LPR never develop cancer, even after decades of reflux symptoms. Those who do develop cancer typically have had unmanaged or poorly controlled reflux for extended periods. The severity and frequency of acid exposure play crucial roles in determining whether and how quickly cellular changes progress. Someone with occasional mild LPR symptoms has substantially different cancer risk compared to someone experiencing severe daily reflux.
Age at diagnosis also influences the timeline significantly. Younger patients with LPR have more years of potential acid exposure ahead of them, potentially increasing long-term cancer risk if their condition remains uncontrolled. Conversely, older patients with newly diagnosed LPR may have less time for cancerous changes to develop. This age-related factor is why medical professionals emphasize early intervention and consistent management regardless of patient age. The concept that “time converts reflux into cancer” is somewhat accurate, but it’s more precise to say that chronic, unmanaged reflux over extended periods increases cancer risk substantially.
Cellular Damage and Barrett’s Esophagus Development
Barrett’s esophagus represents a critical milestone in understanding how LPR progresses toward potential cancer. This condition occurs when the normal squamous epithelium lining the esophagus, larynx, and pharynx transforms into columnar epithelium similar to stomach tissue. This metaplastic change is the body’s attempt to protect delicate tissues from repeated acid exposure, but it represents a pre-cancerous condition. Patients with Barrett’s esophagus have significantly increased risk of developing esophageal adenocarcinoma, though most Barrett’s patients never develop cancer.
The development of Barrett’s esophagus from chronic LPR typically requires years of acid exposure. Research indicates that Barrett’s development occurs in approximately 10-15% of patients with chronic GERD, and rates are likely similar for LPR patients, though specific LPR statistics are less extensively documented. Once Barrett’s esophagus develops, the risk of progression to dysplasia and eventually cancer increases, but progression is not inevitable. Regular endoscopic surveillance allows physicians to monitor for dysplastic changes and intervene before cancer develops.
Dysplasia—abnormal cell growth within Barrett’s tissue—represents the next step toward potential malignancy. Low-grade dysplasia, where cells show some abnormality but retain relatively normal architecture, progresses to high-grade dysplasia or cancer at varying rates. Some low-grade dysplasia cases remain stable for years, while others progress more rapidly. This unpredictability is why medical professionals recommend different surveillance intervals based on dysplasia severity. Understanding these cellular changes helps explain why LPR doesn’t automatically cause cancer, but why chronic unmanaged reflux increases cancer risk progressively over time.
Risk Factors That Increase Cancer Potential
Several factors dramatically influence whether chronic LPR progresses toward cancer. Smoking represents one of the most significant modifiable risk factors. Tobacco smoke damages the protective mechanisms in throat tissue and synergizes with acid damage to dramatically increase cancer risk. The combination of smoking and chronic reflux creates a particularly dangerous environment for cellular transformation. Patients with LPR who smoke have substantially higher cancer rates than non-smoking LPR patients, making smoking cessation critically important for reflux sufferers.
Alcohol consumption similarly elevates cancer risk in patients with chronic reflux. Alcohol damages the esophageal lining, relaxes the lower esophageal sphincter, and impairs the body’s ability to repair acid damage. Heavy alcohol use combined with LPR creates a compounding effect on cancer risk. Obesity also plays a significant role, as excess abdominal weight increases intra-abdominal pressure, forcing stomach contents upward and worsening reflux. Weight management becomes part of cancer prevention strategy for obese patients with LPR.
Helicobacter pylori infection, a bacterial infection affecting the stomach, interacts with reflux disease in complex ways affecting cancer risk. Poor dietary choices, particularly diets low in fruits and vegetables, reduce the body’s antioxidant defenses against cellular damage. Male gender and advancing age are non-modifiable risk factors that increase cancer risk in reflux patients. Genetic predisposition also plays a role; some families have higher rates of reflux-related cancers. Understanding these risk factors allows patients and physicians to identify high-risk individuals who require more aggressive monitoring and management.
Prevention and Management Strategies
Effective LPR management significantly reduces cancer risk by preventing chronic acid exposure. Proton pump inhibitors (PPIs) and H2-receptor antagonists reduce stomach acid production and are the primary pharmacological treatments for LPR. Regular use of these medications allows damaged tissue to heal and prevents continued irritation. However, medication alone is insufficient; lifestyle modifications provide essential complementary benefits. Elevating the head of your bed, avoiding eating within three hours of sleep, and eliminating trigger foods all reduce reflux frequency and severity.
Dietary modifications represent crucial prevention strategies. Eliminating or reducing spicy foods, citrus fruits, tomato-based products, chocolate, caffeine, and alcohol helps minimize reflux episodes. Eating smaller, more frequent meals rather than large meals reduces pressure on the lower esophageal sphincter. Maintaining a healthy weight through exercise and balanced nutrition reduces abdominal pressure contributing to reflux. These lifestyle changes, while sometimes challenging, offer substantial long-term benefits in reducing acid exposure and associated cancer risk.
Regular medical monitoring through endoscopy allows early detection of Barrett’s esophagus or dysplastic changes before they progress to cancer. Patients with chronic LPR should work with gastroenterologists to establish appropriate surveillance intervals based on individual risk factors. For those developing Barrett’s esophagus, more frequent monitoring becomes necessary. Some patients with high-grade dysplasia benefit from endoscopic interventions like radiofrequency ablation or endoscopic mucosal resection, which can eliminate pre-cancerous tissue before malignant transformation occurs. These preventive approaches have dramatically improved outcomes for reflux patients.
When to Seek Medical Evaluation
Patients experiencing persistent LPR symptoms should seek medical evaluation promptly, particularly if symptoms persist despite over-the-counter antacid use or lifestyle modifications. Chronic hoarseness lasting more than two weeks, persistent throat clearing, difficulty swallowing, or sensation of a lump in the throat warrants professional assessment. Early diagnosis and treatment of LPR allows physicians to prevent progression and reduce long-term complications including cancer risk. Don’t assume that throat symptoms are simply due to allergies or temporary irritation if they persist for extended periods.
If you have been diagnosed with LPR, consistent follow-up with your healthcare provider is essential. Report any changes in symptoms, new symptoms, or concerns about medication side effects. If you develop additional risk factors like smoking initiation or significant weight gain, inform your physician as these may necessitate more aggressive management or surveillance. For patients with Barrett’s esophagus, adherence to recommended endoscopic surveillance schedules is critical for early detection of dysplastic changes. These preventive medical approaches, combined with diligent home management, provide the best protection against LPR-related cancer development.
Consider consulting a gastroenterologist if your primary care physician diagnoses LPR, particularly if you have multiple cancer risk factors. Specialists can provide detailed assessment of your individual cancer risk, recommend appropriate surveillance intervals, and discuss advanced treatment options if needed. Documentation of your reflux history becomes important for tracking disease progression over time. By taking an active role in your healthcare and maintaining regular medical contact, you significantly improve your ability to prevent serious complications from chronic LPR.
FAQ
Does everyone with LPR develop cancer?
No. The vast majority of people with LPR never develop cancer, even with long-standing reflux. Cancer development requires a combination of chronic, unmanaged reflux plus additional risk factors. Patients who actively manage their LPR through medication and lifestyle changes have substantially lower cancer risk. Many people live decades with LPR without ever developing malignancy, particularly when their condition is well-controlled.
How quickly can LPR progress to cancer?
Cancer development from LPR is not a rapid process. The progression from normal tissue to Barrett’s esophagus typically requires years, and further progression from Barrett’s to dysplasia and cancer takes additional years or decades. Most research suggests that significant cancer risk develops only after many years of chronic, poorly managed reflux. This extended timeline provides substantial opportunity for early detection and intervention before malignancy develops.
What are the warning signs that LPR is becoming serious?
Warning signs include difficulty swallowing that worsens progressively, unintentional weight loss, persistent pain in the throat or chest, vomiting blood, or black/tarry stools. These symptoms suggest possible progression beyond simple reflux and warrant immediate medical evaluation. Additionally, if you develop new symptoms despite taking reflux medications, or if your symptoms change in character, contact your physician promptly.
Can medication prevent LPR-related cancer?
Medications like proton pump inhibitors reduce acid exposure and allow tissue to heal, substantially lowering cancer risk. However, medication alone is not sufficient; lifestyle modifications, smoking cessation, weight management, and dietary changes all play important roles. The combination of consistent medication use, lifestyle changes, and regular medical monitoring provides the best cancer prevention approach for LPR patients.
How often should someone with LPR have endoscopy screening?
Screening frequency depends on individual risk factors and whether Barrett’s esophagus has been diagnosed. Patients with uncomplicated LPR may not require routine endoscopy if symptoms are well-controlled. Those with Barrett’s esophagus typically need surveillance every 2-5 years depending on dysplasia presence and severity. Your gastroenterologist will recommend appropriate screening intervals based on your specific situation. The American Society for Gastrointestinal Endoscopy provides evidence-based guidelines for surveillance recommendations.
Is LPR-related cancer preventable?
LPR-related cancer is largely preventable through aggressive management of reflux symptoms. Early diagnosis, consistent medication use, lifestyle modifications, smoking cessation, and regular medical monitoring all significantly reduce cancer risk. While some individuals may have genetic predispositions to cancer development, environmental and behavioral factors remain modifiable. By taking an active role in managing your LPR, you substantially decrease the likelihood of developing reflux-related malignancy.


